Deutsche AIDS-Hilfe is the oldest German organization dealing with HIV preventive treatment among vulnerable groups. The non-profit organization has 130 divisions throughout the country. AIDS.CENTER reporters spoke with Tatiana Gangarova, a specialist on working with migrants, about HIV preventive treatment among refugees, social projects, working with communities and discrimination.
How was your organization created and how does it work now?
Initially, it was founded by a group of HIV positive gay individuals who were fighting for their rights. In addition to them, sex workers and drug users were also participating in this fight. Aids-Hilfe appeared as a result of their union.
Now we are an official NPO and as such, we receive part of our funds from the German government. It has to be said that in our country we have a rather interesting scheme of responsibility in the field of HIV and AIDS. The Federal Ministry of Health allocates money to the Federal Centre for Health Education, which deals with the general population, including preventive treatment programs for adolescents. And our task is to work with key groups: preventive treatment among gays, migrants and refugees, sex workers, injecting drug users, and prisoners. We are not working with people outside these groups. But, unlike the state, it is much easier for us to work with them, as we are part of them, and it is much easier for us to get inside this or that community.
How exactly is your work with key groups organized?
Each particular group has its specific language. And the way we speak, for example, with gays, is significantly different from a similar conversation with refugees. They have different needs, and we work with them in different ways.
Moreover, we try to involve the communities themselves in the study of methods of organizing preventive treatment and the use of such techniques as mapping, storytelling through photos (photovoice), theatre and so on. These alternative techniques allow us to involve people in our projects, even if they speak neither German nor English. Using these methods, they can express themselves through images or tell stories, for example, in Arabic, which we can translate and use in our work later. It is a kind of collective production of knowledge, through which our campaigns for migrants, sex workers or drug users are actually developed by the communities themselves, right down to the smallest elements, such as postcards. They decide themselves what images are appropriate and not discriminatory.
One of the key areas of our work is the creation of platforms for the self-organization of communities, on the basis of which they can be integrated into political activities in the future. Because it is impossible to carry out HIV preventive treatment without expressing one's position against the criminalization of sex workers and drug users.
For example, it is impossible to help refugees without fighting racism and discrimination in the country. It is necessary to take into account that 24 out of 82 million people living in Germany have a migratory background. Many refugees enter the country illegally, without any documents. And there is no medicine for them and that is just wrong. So we also have to carry out a political campaign so that such people have access to treatment.
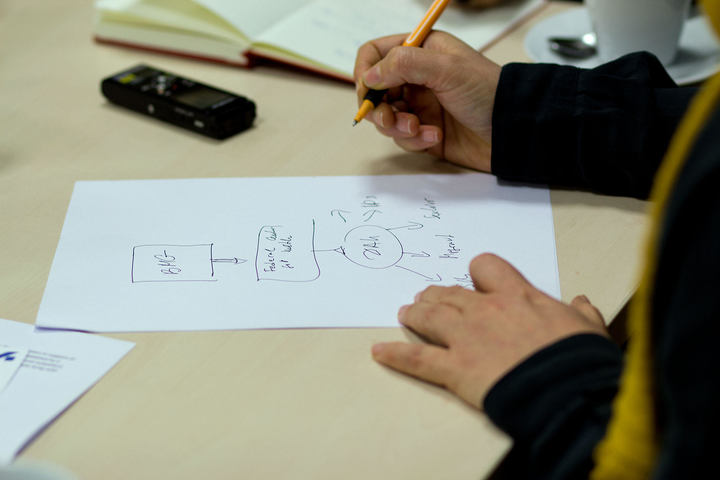
The scheme of responsibility for HIV preventive treatment in Germany. The Federal Ministry of Health allocates money to the Federal Centre for Health Education and it transfers the funds to non-profit organizations. Photo: Fedya Ily
And what about access to treatment among refugees in general? Is it easy to get?
In Germany, by law, a refugee receives insurance, which provides a rather limited access to health services. In particular, it includes emergency cases and everything related to pregnancy. The law includes the wording: 'In the long term, without proper treatment HIV can lead to death', so that this insurance also extends to antiretroviral therapy.
However, if the reason for the request for asylum was specifically HIV infection, then it is necessary to confirm that in his or her native country the person did not have access to this treatment. For example, if a person arrives from Senegal requesting asylum because he or she was not able to receive treatment there, and Senegal itself contends that there is treatment, then the migrant can be sent back.
But it is hardly the case that all refugees with HIV are going to Germany in the hope of receiving treatment.
Yes. It has to be understood that almost all refugees have far from only one reason to seek asylum. It is impossible to guess: whether a person with HIV will be allowed to enter the country or not. Many come without knowing their status. And in most cases, refugees are not coming because they need therapy. You must admit that it is difficult to refuse asylum to a person because of their HIV status if he or she is on a hit list in his or her country.
The majority come for political reasons, some were persecuted back home because of their sexual orientation. For example, a large number of drug-related harm reduction activists come from Russia, because they have been persecuted in their homeland. When they file documents for asylum here, of course they are given treatment, because this is a matter of basic human rights.
What happens after an asylum request?
'It is impossible to help refugees without fighting racism and discrimination in the country. 24 out of 82 million people living in Germany have a migratory background'.
They have to confirm that the situation from which they are fleeing did, indeed, take place. Without this, many are sent back. If the request for asylum is denied, the next step is deportation. But still many stay, as they do not want to go back. They are difficult to judge, because, after all, a person has the right to migrate. But then they find themselves in a very sticky situation: no documents means no legal work and no legal treatment. Unfortunately, we really cannot offer a solution for them. Although we have organized protests in order to draw attention to this problem, each state is focused on its own security, and they need to know about everyone who lives in the country. They do not want to create any model for providing treatment to people without documents, because they are not interested in those people staying here.
Of course, there are some doctors who stash pills at their own risk and give them to people, but it cannot be continued on an ongoing basis. These doctors are real fighters for human rights, but by doing so they commit a criminal offence. As you can see, Germany is a very democratic and wealthy country, but at the same time, we have practically no options for some groups of people. And this is a huge problem.
Tatyana Gangarova shows an example of a card with a refugee story. . Photo: Fedya Ily
In Germany, PrEP is very widely used for HIV preventive treatment, but is it possible for migrants to get access to it?
There is already information that in the future doctors will officially prescribe it, but even now it is very cheap by German standards – about 40-50 euros. Moreover, in Germany, there are check-points with free PrEP for those who cannot afford to buy it. However, the problem with refugees who have no documents still remains. Because when you come to these check-points, you are still asked for documents to confirm the legality of your presence in the country. If you have no documents, you will not get PrEP. So it is also not a solution for everyone.
Is there any different way to spread information about HIV among refugees? And in the perception of the refugees themselves?
Definitely. For example, the simple distribution of flyers does not work at all. Most of them will never take a flyer because the word AIDS is written everywhere on it. They are afraid that their relatives will suspect them even because of a simple interest in this topic. Thus, more often they prefer to look for information on the Internet.
Or there is our largest project, established in cooperation with African churches. Only in Berlin, there are 118 such parishes. Our colleagues go there once a month, talk about HIV and preventive treatment, and also offer HIV tests. However, there is also a problem: people simply refuse to take medicine, they are convinced that God will punish them for it. And it is very dangerous. Especially for such cases, we have developed a brochure for African pastors, which literally says the following: 'Okay, God has given us the knowledge to invent pills, so it is the God’s will that you take them and pray'. And that really works, because now this idea is broadcast by the pastor.
I do not personally belong to any religious group, but if you want to work with religious people, then you have to respect their faith. Respecting someone else's opinion, in this case, is the main reason why this project is successful, and the World Health Organization (WHO) even included it in the top 20 projects in 2018.
Office of Deutsche AIDS-Hilfe in Berlin. Photo: Fedya Ily
You have mentioned alternative methods of working with migrants who do not speak German and English. What are they like?
My favourite project is photovoice (storytelling through photos), in which refugees tell stories about their experience, about their feelings. We collect these stories and then publish them on our website and in a hard copy version in at least 6 languages, including Russian. It helps to convey information.
For example, a story of discrimination by a doctor. An HIV-positive refugee came to the German doctor and said: 'I just recently came and I don’t speak German yet, I can only speak English'. Usually, doctors know that refugees do not always speak German, but the doctor looked at him and answered: 'Everyone in Germany must speak German'. And the guy was shocked. He went to the doctor for help, in the end, he was very upset.
And the story shown on this postcard is my favourite. The woman is wearing a hijab, and she was sent to a local HIV service organization, in which most of the employees are gay and, accordingly, are used to working almost exclusively with other gay people. And they ask her: 'Pardon, what are you doing here? The Arabic shop is across the road!' She began to explain that she was also HIV-positive, but she was not believed, simply because she had on a hijab. She wondered for a long time after that: 'Is such an attitude just because I am an Arab woman? Yes, I am an Arab woman and also I have sex!' At the same time, she is a pretty broad-minded person.
Office of Deutsche AIDS-Hilfe in Berlin. Photo: Fedya Ily
And how do you work with theatre?
We have two migrant troupes, they travel and perform at refugee camps. One refugee from Algeria with an art education asked us for funding, and together with the local Academy of Arts we helped out: now a coach comes to them and helps with staging and script writing. What is more, their performances are based on the personal experience of the actors. At first, I was worried that they would be afraid to reveal their status in performances, but they said: 'On the stage we are actors! And we could play anyone, Tanya'.
At the same time, they integrate images into the set, because if you just ask a person: 'Have you ever experienced discrimination or stigmatization in Germany?', no one will answer 'Yes', just because these are intangible concepts, and sometimes it is difficult to define them. But if you ask: 'What made you upset?', they will definitely tell you. We ask them to take a photo of what upset them. And using these photos we can talk about discrimination.
Once a woman brought a photo of an apple, and the whole group began to laugh, saying, how is it even possible for an apple to upset someone? And then she said that she moved to Germany when she was pregnant and was living in a refugee camp. She was tested for HIV, and it turned out that she was HIV-positive. At that time, the refugees were still given bags of food, not money to buy food. They were not asked what they wanted to eat. And every day there was an apple in this bag. Apples do not grow in her homeland, and she'd dreamed of trying them, but suddenly she was eating apples every day for 5 months. Finally, she asked for at least one banana, but the next day they brought a bag with an apple again. This story is a good example of structural discrimination. Nevertheless, this woman would never say that she was discriminated against in this way. Now the troupe is already ten years old, and they are really successful.
Photo of an apple, made by a refugee from the theatre troupe.. Photo: Fedya Ily
There are many areas in our work: we have peer counseling educational programs for migrants, our own media, we design websites for each at-risk group and we conduct anti-discrimination campaigns. All of these programs serve as preventive treatment in a much wider and inclusive sense.
Этот материал подготовила для вас редакция фонда. Мы существуем благодаря вашей помощи. Вы можете помочь нам прямо сейчас.